|
1
|
- Kenneth Fine, M.D.
Intestinal Health Institute
- Dallas, TX
|
|
2
|
|
|
3
|
- Symptoms/Signs
- “Patients have eructations, flatulence and heavy pains of the stomach”
- “They are emaciated and atrophied, pale, feeble, incapable of performing
any of their accustomed work”
- “The stomach labors in digestion when diarrhea, consisting of undigested
food in a fluid state, seizes the patient”
|
|
4
|
- “Errors in diet may perhaps be a cause.....
- to regulate the food is the
main part of treatment”
- “The allowance of farinaceous food must be
small; highly starchy food, rice, sago, corn
flour are unfit”
- “Malted food is better, also rusks or bread cut
thin and well toasted on both sides”
|
|
5
|
|
|
6
|
- Celiac disease is caused by the harmful
- effects of wheat, barley, rye, and oat flour
- It is gliadin, an alcohol soluble subfraction of gluten, that is the
deleterious factor (not starch)
- Following removal of gluten from the diet, there is a time lag before
symptoms disappear, or reappear with its re-introduction
|
|
7
|
- Symptoms or signs due to malabsorption of fluid, electrolytes, and/or
nutrients
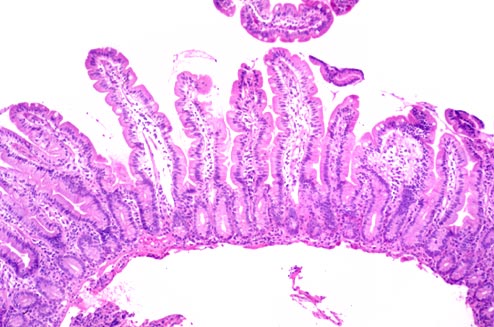
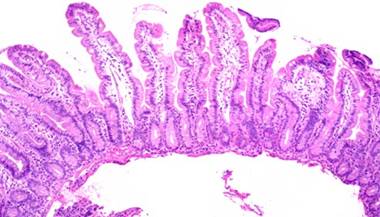
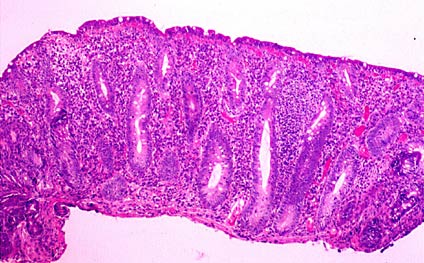
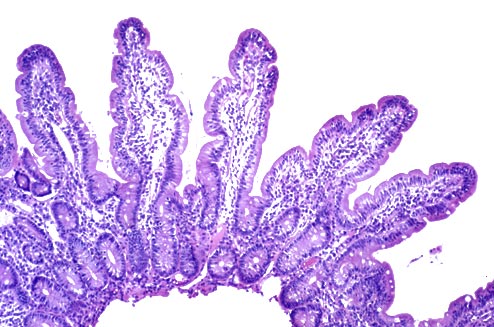
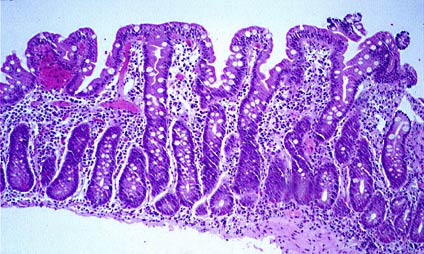
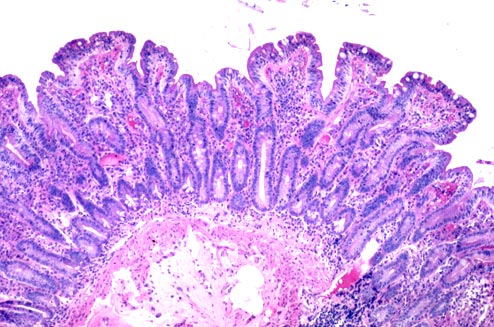
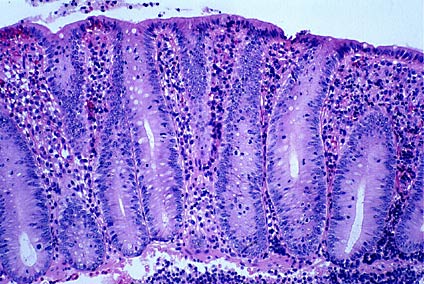
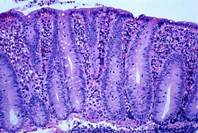
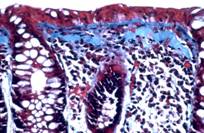
- Small intestinal histopathology
- Inflammation of lamina propria
- Intraepithelial lymphocytosis
- Villous atrophy
- Crypt hyperplasia
- Clinical improvement with gluten-free diet
|
|
8
|
- Abdominal - diarrhea, gas, bloating, nausea, vomiting, fat in stool,
constipation
- Musculoskeletal - weakness, muscle spasms, bone pain, numbness,
osteoporosis, low calcium
- Blood - anemia, high platelets,
low clotting factors
- Associated diseases - autoimmune, microscopic colitis, Crohn’s disease,
low pancreatic enzymes, dermatitis herpetiformis, lymphoma, cancer
|
|
9
|
- Clinical presentation
- Asymptomatic (with or without iron deficiency)
- Abdominal bloating, nausea, G-E reflux
- Diarrhea, weight loss, symptoms of fat malabsorption
- Histopathology
- Mild intraepithelial lymphocytosis or plasmacytosis of LP, normal villi
and crypts (May be read as
normal)
- Partial or subtotal villous atrophy and inflammation
- Total villous atrophy, inflammation, crypt hyperplasia
|
|
10
|
|
|
11
|
|
|
12
|
|
|
13
|
- Ancient times - clinical observation
- 1950-1960’s - response to gluten free diet, 72-hr
fecal fat, low xylose test, origins of SB biopsy
- 1970’s - Anti-gluten Ab in blood / intestinal fluid
- 1980’s - Antigliadin / antiendomysial Ab in blood
- 1990’s - Antitissue transglutaminse Ab
- Mistakenly thought to rule in
and rule out all disease
|
|
14
|
- Patients cannot have gluten sensitivity/celiac sprue:
- If they have not lost weight
- If they are obese
- If they have no intestinal symptoms
- If they are elderly
- If they have negative screening blood tests
- If they have no steatorrhea
- If they have a normal small bowel biopsy
|
|
15
|
- Celiac sprue is the end-stage of immunologic gluten sensitivity directed
at the small intestine
- HLA genes (HLA-DQ2, DQ8) direct gluten-induced damage to SB; other
HLA/non-HLA genes damage skin (e.g. DH and/or other organs
- Blood tests/biopsies can only diagnose celiac sprue
- GS with mild/no SB damage; autoimmune disease of other organs; relatives
of celiacs are being missed
|
|
16
|
- “Gluten-Sensitive Diarrhea” (Gastroenterology 1980;79:801)
- 8 females, severe chronic diarrhea,normal blood and stool tests
- “Gluten-Sensitivity with Mild Enteropathy” (Gastro 1996;111:608)
- 10 pts. diarrhea/steatorrhea, anemia, osteoporosis, mouth ulcers
- Small bowel biopsies reacted immunologically to gluten in vitro
- “Celiac-like Abnormalities in IBS patients” (Gastro 2001;121:1329)
- Small intestinal antigliadin IgA Ab, HLA-DQ2 in 30% of IBS pts
- “Celiac Disease without Villous Atrophy”
(Dig Dis Sci 2001;46:879)
- 10 pts. with abdominal symptoms, osteoporosis, (-* IEL’s
- All pts. became well on GFD; recurred with gluten
|
|
17
|
- Two research groups tested 69 or 89 untreated celiacs, and 16 first
degree relatives
- Serum antigliadin and antiendomysial IgA antibody
- Each test positive in only 59% of celiacs
- One or the other test positive in only 76-78%
- Positivity dependent on degree of villous atrophy (VA)
- Partial VA - 31% Subtotal VA -
70% Total VA - 100%
- Relatives - mild SB inflammation; all tests negative
|
|
18
|
|
|
19
|
- Diabetes mellitus, type 1
- Dermatitis herpetiformis
- Alopecia
- Sjogren’s syndrome, rheumatoid arthritis, others
- Thyroiditis
- Autoimmune hepatitis, PBC
- Psoriasis
- Microscopic colitis
|
|
20
|
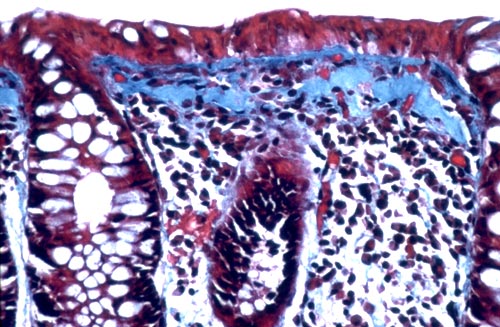
- Chronic, watery, non-bloody diarrhea
- Normal/near normal colonoscopy
- May have patchy edema, loss of vascularity, erythema, occasional
mucosal fracture
- Abnormal colonic biopsy
- Lamina propria inflammation
- Intraepithelial lymphocytosis
- Surface epithelial flattening
- +/- thick subepithelial collagen band
|
|
21
|
|
|
22
|
- 64% have DQ2; most remainder have DQ1,3
- 70% have mild SB enteropathy but rarely CS
- No more antigliadin antibody in serum than general population
- Histopathology of MC in colon identical to celiac sprue in small
intestine
|
|
23
|
- Researchers assessed blood and aspirated small bowel fluid for
antigliadin IgA antibody in:
- Celiacs; blood and SB aspirate was positive
- Normals; blood and SB aspirate was negative
- Celiacs after 1 yr on GFD; blood was negative, intestine was positive
when mild SB inflammation persisted
- Used intestinal lavage and analysis of rectal effluent to test for the
presence of intestinal antigliadin Ab
- Called “a relatively non-invasive screening method for early celiac
sprue”
|
|
24
|
|
|
25
|
- Offered access to fecal testing for gluten/food sensitivity,
malabsorption, colitis to the public and medical practitioners on the
Internet
- Tracked clinical information, results of tests
- Followed up by online survey
- Aim: to bring the benefits of medical research to the public while
ongoing research, and public/medical education are underway (years)
|
|
26
|
|
|
27
|
- 42% have autoimmune disease
- 21% have IBS symptoms
- 20% have family history of celiac/GS
- 6% have microscopic colitis
- 2% have chronic fatigue
- 8% have wt. loss, headaches, allergies, seizures, osteoporosis,
neuropathy, autism, ADD/ADHD
- Only 0.6% have no symptoms or identified risk
|
|
28
|
- 99.4% Sick/Symtpomatic
- 57% have HLA-DQ2 or DQ8 (celiac genes)
- 42% in general U.S. population
- Only 0.07% have no predisposing gene
- 0.4% of general U.S. population
- 60% positive for gluten sensitivity
- Highest gliadin values (>200) with DQ2,8,7 in 88%
- 60% in general U.S. population
|
|
29
|
|
|
30
|
|
|
31
|
|
|
32
|
|
|
33
|
- First report, a letter from France 1994 (Clin Lab)
- 10 patients with CS had detectable AGA in stool
- 2 did not have it in serum
- 2002, Italian study showing AGA and AEA in 21 CS patients, 10 treated CS
after challenge (Am J Gastro)
- “Proved intestinal mucosa produces Ab”
- Did correlates of biopsies reacting to gliadin in vivo
|
|
34
|
- 2004 German Study found higher fecal AGA in 26 CS than 167 healthy
controls (Clin Lab)
- 2006 German Study of 20 celiac kids (BMJ)
- Did not alter serum method or calculation of positive
- 10% sensitive, 98% specific
- If used a lower cut off, was 82% sensitive, 58% specific
- Only applied to CS, not gluten sensitivity
|
|
35
|
- Amount sample is diluted prior to analysis
- Technique/amount of washing of ELISA plates
- Greater solid contaminant of fecal fluid vs. serum
- Mathematical conversion of OD to a Unit
- How calculated Unit is interpreted: norm vs. abnorm
- Centrifuge speed for stool (too high
neg result)
- Proper collection and preservation of stool
|
|
36
|
- DQ1,3 found more commonly in MC and RA
- DQ3 subtypes are: DQ7, DQ8, DQ9
- DQ1 found more commonly in gluten ataxia
- DQ9 binds and reacts to gluten in vitro
- Only DQ4 seems not to increase risk of GS
- Rare in U.S. - 13% heterozygous, 0.4% homo.
|
|
37
|
- 100 A.D. - 1950 - clinical observation
- 1950 -1960’s - response to gluten free diet, 72-hr
fecal fat, oral xylose test, origins of SB biopsy
- 1980 -1990’s - serologic testing for antigliadin Ab, antiendomysial Ab,
antitissue transglutaminase Ab
- 2000’s - fecal testing for Antigliadin Ab and Antitissue
transglutaminase Ab†; Quantitative fecal fat microscopy for
malabsorption†; HLA-DQ typing
|
|
38
|
- New method of fecal fat microscopy allowing quantitation of fecal fat
output from a single stool
- Easily diagnoses intestinal nutrient malabsorption and establishes a
numeric pretreatment baseline
- Correlates with quantitative fecal fat excretion measured in 72-hour
stool collections
- More sensitive than qualitative fecal fat & 72-hour collections (30-50%
do not collect all stools)
|
|
39
|
|
|
40
|
- Stool for Antibody and Malabsorption Testing
- Fecal antigliadin and antitissue transglutaminase IgA
- Quantitative fecal fat microscopy
- Swab of inside of mouth for Gene Testing
- HLA-DQB1 typing for gluten
sensitive/celiac genes
- Other tests available: Fecal anti-casein, anti-ovalbumin, anti-Saccharomyces
cerevisiae, anti-soy IgA for
dietary milk, egg, yeast and soy sensitivity; fecal lactoferrin for
acute or chronic colitis;
extensive food sensitivity panel coming soon
|
|
41
|
- Microscopic colitis, Crohn’s, UC, any IBD
- Relatives of gluten-sensitive individuals
- Chronic diarrhea of unknown origin
- Irritable bowel syndrome
- Inflammatory bowel disease
- Gastroesophageal reflux disease
- Hepatitis C, Autoimmune/other liver disease
- Short stature in children, Down's syndrome
|
|
42
|
- Female infertility, mother of spina bifida
- Peripheral neuropathy,Seizure disorders
- Psychiatric Dz, Depression, Autism
- Diabetes mellitus, type 1, type 2 (?)
- Rheumatoid arthritis, Sjogren's syndrome, Lupus, Autoimmune thyroid
disease, Any autoimmune Dz
- Asthma, AIDS, Osteoporosis, Iron deficiency
- Everyone!
|
|
43
|
- Stop NSAID’s (including aspirin), anti-acid Rx
- Fecal fat test
- Fecal AGA IgA; ATTA IgA
- GFD if positive or as trial
- Lactobacillus GG 1 BID-TID
- No response – wash out gut, cholestyramine, stop estrogen, BSS
- Bismuth subsalicylate tablets 3 tid for 8 weeks
|
|
44
|
- Intestinal Health Institute (not-for-profit
institute)
- Medical research, education, public service
- http://www.intestinalhealth.org
- FinerHealth and Nutrition
- Free online educational information
- http://www.finerhealth.com
- EnteroLab.com
- Breakthrough diagnostic testing available, affordable
- http://www.enterolab.com
- The Organic Alternative.com (coming soon)
- Affordable organic dried fruit, nuts, health products http://www.theorganicalternative.com
|
 Notes
Notes{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}